
Urinary incontinence is the inability to hold urine even till reaching the toilet. 1 in 10
women experience urinary incontinence. It is often temporary. (In this fact sheet, the term
"incontinence" will be used to mean urinary incontinence.)
Women experience incontinence twice as often as men. Pregnancy and childbirth, menopause,
and the stricture of the female urinary tract account for this difference. But, both women
and men can become incontinent from neurologic injury, birth defects, strokes, multiple
sclerosis, and physical problems associated with aging.
Older women experience incontinence more often than younger women. But, incontinence is not
inevitable with age. Incontinence is treatable and often curable at all ages. If you
experience incontinence, you may feel embarrassed. You will need to overcome your
embarrassment and see a doctor to learn if you need treatment for an underlying medical
condition.
Incontinence in women usually occurs because of problems with muscles that help to hold or
release urine. The body stores urinein the bladder, which is a balloon-like organ. The
bladder connects to the urethra, the tube through which urine leaves the body.
During urination, muscles of the bladder wall contract and force urine out of the bladder
and into the urethra. At the same time, sphincter muscles surrounding the urethra relax and
let urine pass out of the body. Incontinence occurs if the bladder muscles contract suddenly
or when the muscles surrounding the urethra relax suddenly.

VVF is an abnormal communication between vagina and urinary bladder leading to continuous leakage of urine. It is mostly after abdominal hysterectomy, Cesarean section, Obstructed labour.

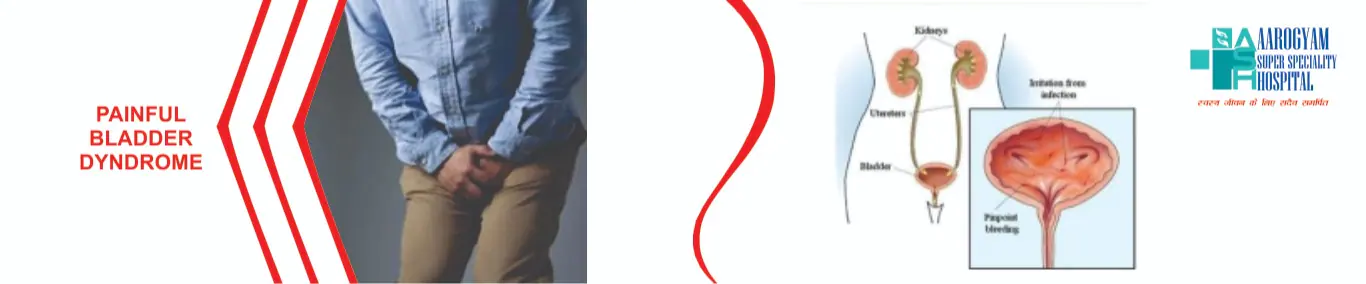
It implies frequency, and urgency of urination with or without urinary leakage. Treated mostly by medications- Anticholinergics, Cystodistension and Intradetrusor BOTOX injection is given for resistant OAB.

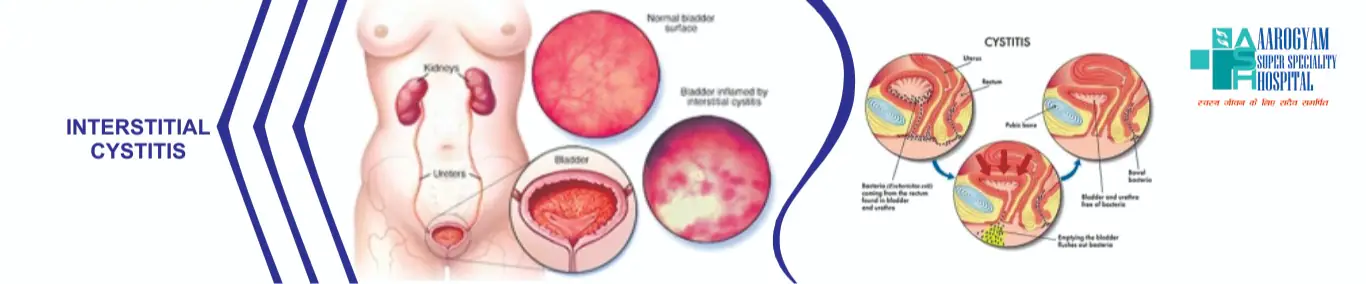
Continuous pain with pressure is there and it increases as the bladder fills. The pain radiates to the lower body parts such as lower abdomen, lower back, urethra or perineal area.
It starts with increased urination and the frequency also increases with the progression of
interstitial cystitis, the frequency is same in day and night.
Urgency to urinate is the most common symptom and sometimes patient feels the need to
urinate even when he/she has urinated
Sometimes people with urinary incontinence faces issues of urine leakage even during sexual
intercourse.
Urinary incontinence is more common in females than males, its chances of acquiring it
increases with age.
It can be due to the following:
The immune system attacks the bladder like in the cases of autoimmune conditions
If there is a defect in urinary bladder due to which the bladder is irritated.
Substances in urine which damages the bladder.
Changes in the blood and nerve supply which carries pain sensation becomes sensitive.
Most Urinary tract infections are caused by micro organism that comes in contact with urinary tract system through your urethra and then the bladder. It happens when bacteria affects the system which carries urine out of the body -- the kidneys, bladder, and the tubes that interface them.
Factors that increase the risk of growing UTI include:
Having a bladder or kidney infection in the past 10 to 12 months
Having diabetes
Having sex frequently with new sex partner

Urethritis – Infection of the urethra
Cystitis – Infection of the bladder
Pyelonephritis – Infection of the kidneys
Strong and frequent urge to urinate
Bloody or dark urine with strong smell
Burning sensation while urinating
Pain in lower back or below the ribs
Pain in your bladder region
Muscle aches and abdominal pains.
Nausea
Vomiting
Chills
High fever
Fatigue
A person having Kidney infection (Pyelonephritis) can experience:
Chills
Fever
Pain in the back
In children, following symptoms will be noticed:
Fever
Vomiting
Irritability or fussiness
Less active
Stomach pain
Back pain
Excessive crying that cannot be resolved by typical measures (e.g feeding, holding)
Drink 8 to 10 glasses of water a day
Don′t control, urinate as soon as you feel the need
Take showers instead of baths
Females should wipe from front to back after urinating
Avoid the use of douches or feminine hygiene sprays
Loose fitting clothes to promote air circulation
Interstitial cystitis/bladder pain syndrome(IC/BPS)is a group of symptoms, including mild to severe bladder pain and an urgent and/or frequent need to urinate. The disorder can affect women and men but is more common in women. It can be difficult to diagnose and treat because the underlying cause is not well understood.
The definition of interstitial cystitis/bladder pain syndrome (IC/BPS) has evolved over the
years, and will probably continue to change as the cause is better understood. The American
Urological Association (AUA) defines IC/BPS as an unpleasant sensation (pain, pressure,
discomfort) perceived to be related to the urinary bladder, associated with lower urinary
tract symptoms of more than six weeks duration, in the absence of infection of other
identifiable causes.
It is difficult to know for sure how many people are affected by IC/BPS, but research
indicates that IC/BPS symptoms occur in about 2 percent of women. However, many fewer than
that are diagnosed with the disorder, perhaps because it is unrecognized.
The symptoms of interstitial cystitis/bladder pain syndrome(IC/BPS)can vary from one person
to another and from one episode to another. All patients with IC/BPS have bladder pain that
is relieved at least partially by urinating. Symptoms usually include a frequent and urgent
need to urinate during the day and/or night. Most, although not all, people with IC/BPS do
not have urinary leakage (incontinence). Most people describe pain in the suprapubic area
(in the lower abdomen, above the pubic bone) or urethral area. The severity of pain ranges
from mild burning to severe and debilitating pelvic pain.
Most people describe symptoms that begin gradually, with worsening discomfort, urgency, and
frequency over a period of months. A smaller subset of patients describes symptoms that are
severe from the beginning. When symptoms of IC/BPS begin suddenly, some patients are able to
name the exact date on which symptoms began.
Some people with IC/BPS also have other types of chronic pain, such as irritable bowel
syndrome, painful menstrual periods, endometriosis, vulvar pain (vulvodynia), fibromyalgia,
or prostatitis. IC/BPS symptoms are sometimes at their worst during times when other pain
symptoms are also at their worst.
Symptoms may vary from one day to the next. Worsening of IC/BPS symptoms may occur after
consuming certain foods or drinks (eg, coffee, alcoholic drinks, spicy foods), during the
luteal phase of the menstrual cycle (14 to 28 days after the first day of the last period),
during stressful times, or after activities such as exercise, sexual intercourse, or bein
The diagnosis of interstitial cystitis/bladder pain syndrome(IC/BPS)is based upon a person′s
symptoms and examination. A careful medical history, physical examination, and sometimes
laboratory testing are needed to confirm the diagnosis and also to be sure that another
condition (eg, bladder infection or kidney stone) is not the cause of symptoms. There is no
single test that can definitively diagnose IC/BPS.
Physical examination: The physical examination usually includes a complete pelvic
examination with a brief rectal exam. Often, patients with IC/BPS have tenderness in the
lower abdomen, hips, and buttocks. Women often have tenderness in the vagina and around the
bladder, and men may have tenderness in the scrotum and penis. For this reason, being
examined can be uncomfortable.
If an examination is too uncomfortable, some healthcare providers will recommend that the
patient begin a course of treatment for IC/BPS without further testing. If improvement is
not seen, it may be necessary to perform more testing to confirm the diagnosis.
Some providers will measure the amount of urine remaining in the bladder after the patient
urinates; this is called a post-void residual. This measurement can be done by inserting a
small catheter into the bladder or by using ultrasound. While it is normal to have some
urine in the bladder after voiding, having a large amount of urine is not normal. Urinary
retention is the medical term for retaining urine in the bladder, and is not typical of
IC/BPS.
Laboratory tests Most clinicians will perform a urine test to ensure that a person′s
symptoms are not related to another condition, such as a kidney stone or bladder infection.
If a urinary tract infection is discovered, the person will be treated with antibiotics. If
blood is detected in the urine, further urine and/or diagnostic testing (eg, cystoscopy) may
be recommended.
Cystoscopy Cystoscopy is a test that allows a doctor to examine the inside of the bladder.
Cystoscopy is not required to diagnoseIC/BPS, but may be recommended in certain situations.
Cystoscopy can be done in the office, after a numbing gel is applied inside the urethra. It
can also be done in an operating room while a patient is under anesthesia, sometimes in
combination with other procedures.
To perform cystoscopy, a physician inserts a thin telescope with a camera through the
urethra and into the bladder. The physician examines the inside (lining) of the bladder to
determine if there are any abnormalities. A person with IC/BPS may have either a normal or
abnormal-appearing bladder. If an abnormality is seen, further testing may be
recommended.
The bladder is a hollow organ located in the pelvis, or lower abdomen. The bladder has two
important functions:
It helps to store urine until it is full.
When the bladder becomes full, there is an urge to urinate, and the bladder empties
completely without any leakage.
Urination can be abnormal if the bladder is unable to empty itself fully or empties itself
before one reaches the bathroom. There can also be leakage before or after urination due to
problems with bladder control.
When the conditions of the nervous system affect the bladder, it is called “neurogenic
bladder.” Conditions like stroke, Parkinson’s disease, multiple sclerosis, disc herniation,
and other nervous system abnormalities can result in neurogenic bladder.
There are two major types of bladder control problems that are associated with a neurogenic
bladder. Depending on the nerves involved and nature of the damage, the bladder becomes
either overactive (spastic or hyper-reflexive) orunderactive (flaccid or hypotonic).
People with overactive bladders have little to no control urinating. If the bladder is
overactive, a person might feel a sudden urge to urinate or might go to the bathroom more
often than necessary. An overactive bladder may result in incontinence (the involuntary or
accidental release of urine).
Neurogenic underactive bladders behave in the opposite way. The bladder loses its ability to
empty properly and fills beyond the normal capacity. At a certain point, the pressure of
urine in the bladder overcomes the sphincter muscle’s ability to retain it, and urine leaks
out. Underactive bladders fail to empty completely and hold on to urine.
Several disorders can cause neurogenic bladder, including the following:
· Stroke
· Parkinson’s disease
· Multiple sclerosis
· Spinal cord injuries
· Spinal surgeries
· Trauma/accidents
· Diseases that affect the nervous system
· Central nervous system tumors
· Spinal congenital (present at birth) abnormalities
· Heavy metal poisoning
Underactive bladder may be a complication of diseases such as syphilis, diabetes, and
polio.
The most common symptom of neurogenic bladder is being unable to control urination. Other
symptoms include the following:
a weak or dribbling urinary stream
an inability to urinate or straining to urinate
frequent urination (urinating eight or more times daily)
urgency (a feeling or need to urinate immediately)
painful urination, which may mean there is a urinary tract infection
Your doctor may order several tests of the nervous system and the bladder to diagnose
neurogenic bladder:
Urodynamic studies (bladder function tests) are conducted to measure bladder capacity,
bladder pressures, the flow of urine, and bladder emptying. A cystoscopy may be performed to
examine the inside of the bladder and urethra (the tube through which urine passes) with a
small telescope (cystoscope).
The skull, spine, and urinary tract may be examined with X-rays, computed tomography (CT),
and magnetic resonance imaging (MRI). You may be referred to a Neurologists for
consultation.
The doctor will perform a physical examination and ask about your medical history,
especially about any neurological problems such as back injury, stroke, or other neurologic
diseases.
There are five types of treatment for neurogenic bladder: physical-psychological,
electrical-stimulatory, drug therapy, intermittent self catheterization, and surgery. The
correct treatment is determined by symptoms, type, and extent of nerve damage, and a
thorough discussion with the patient.
Physical-psychological therapy
Physical-psychological therapy, also called timed voiding, combines will power and exercise.
Your doctor will ask you to keep a voiding diary--a record of the amount and time you drink
fluids, how many times you urinate each day, and whether you ever leak urine. This record
creates a pattern that may help you determine the times of the day you should be near a
bathroom, and the times when you should attempt to urinate. The periods of time between
urination gradually get longer and longer as you gain control over urinating.
Electrical-stimulatory therapy: In electrical-stimulatory therapy, electrodes and a small
stimulator are placed near certain nerves during a minor surgical procedure. The stimulator
is placed beneath the skin and delivers electrical impulses that imitate those that are
delivered by normal nerves. The device has been approved by the U.S. Food and Drug
Administration to treat incontinence and urinary retention in patients in whom other
therapies have failed.
Drug therapy
There are certain drugs that reduce muscle spasms and tremors, and other drugs that produce
contractions.
Antispasmodic drugs prevent excessive bladder contractions. Tolteridinetartrate and
oxybutynin chloridework by relaxing the smooth muscle of the bladder.
Antidepressants such as amitryptiline (Elavil) also help to reduce contractions by relaxing
the smooth muscle of the bladder
Estrogen (Premarin) may be used by post-menopausal women to treat mild to moderate stress
incontinence.
Intermittent self-catheterization
Catheters are devices that can be inserted through the urethra and into the bladder to drain
urine. Patients can learn to insert the catheter themselves. This treatment is called Clean
Intermittent Catheterization (CIC).
An indwelling (Foley) catheterization places a catheter in the bladder for an extended
period of time. Catheters prevent bladder swelling by continually draining urine into a
bedside collector. The patient must employ strict sanitary procedures to prevent urinary
tract infection.
Artificial sphincters consist of a cuff that fits around the bladder neck, a
pressure-regulating balloon, and a pump that inflates the cuff. The balloon is placed
beneath the abdominal muscles. The pump is placed in the labia in women and in the scrotum
for men. (Other locations include beneath the skin of the abdominal wall or thigh.)
Activating the pump sends fluid from the cuff to the balloon, allowing the sphincter muscle
to relax and urine to pass. The cuff automatically re-inflates in three to five minutes.
Urinary diversion creates a stoma (opening) through which urine is sent to a collection
pouch.
Bladder augmentation (augmentation cystoplasty)—Segments of the intestine (sigmoid colon)
are removed and attached to the walls of the bladder. This reduces the bladder’s internal
pressure and increases its capacity to store urine.
Urethral stents, which are similar to an internal catheter, can be inserted through the
sphincter muscle to expand it and allow urine to be drained.
The sphincter can be surgically weakened by a procedure called sphincter resection, which
removes a portion of the muscle, or the muscle may be removed completely in a
sphincterotomy.
Although many of these procedures may appear to create a burden, they can prevent kidney
damage. If neurogenic bladder is not treated, it can lead to renal
Cystoscopy is a procedure during which the cystoscope i.e. a thin tube equipped with a camera and light on the end is inserted through the urethra into the bladder to view the urinary tract. The camera captures magnified admincare/images and display on the screen which helps the health care provider for diagnosis.
This test is indicated if you have following symptoms
- Prolonged, continuous urinary problems
- Constant need to urinate
- Painful urination
- Blood in urine
- UTI – Urinary Tract Infection
- Urinary Incontinence - accidental loss of urine
- Urinary Retention- Inability to empty the bladder completely
- Blockages due to Bladder stones
- Enlarged prostate gland
- Noncancerous growths
- Problems with the ureters (tubes) connecting your bladder to the kidneys
- Stricture- narrowing of the urethra, it can be a sign of an enlarged prostate in men
- Polyps or overgrowth of normal tissue
- Cancer or tumor of the bladder
- Injury of the urinary tract
- Abnormalities of the urinary tract that may be present at birth and may lead to a backflow of urine or kidney problems

Take time for yourself, your body needs time for recover
- After cystoscopy include large amount of fluid intake in your routine as it will dilute the urine and reduce urinary discomfort
- Take medications prescribed by the doctor only, avoid excess medications as they might increase the risk of bleeding
- Avoid weight lifting exercises, running for couple of weeks
- Blood in urine is normal after the procedure but if it is continuous than there is a need to visit the doctor
If you have any of the following than visit your doctor:
- Fever or chills
- Lower back pain
- Urinary frequency or urgency
- Inability to urinate
- Continue burning with urination
- Continue blood in the urine